by Dr. Bob Uttl
Dr. Todd Kettner, a registrant of the College of Psychologists of British Columbia (now College of Health and Care Professionals of BC) and a member of Canadian Psychological Association, was the first psychologist Ms. T saw after she was walked out of the class on May 10, 2020, for reasons unknown (the reasons were kept secret by the School District No. 5 Southeast Kootenay administrators).
In rather foggy and unclear circumstances, Ms. T’s physician referred her to Dr. Todd Kettner who was practicing in Nelson, BC, as part of the Summit Psychology, the group he founded. Accordingly, Ms. T made an appointment with Dr. Kettner. Unknown to her, once the SD5 learned about the appointment, the SD5 Director of Human Resources, Ms. Cynthia Stuart, secretly contacted Dr. Kettner and commenced secret ex-parte email communications with Dr. Kettner who reciprocated even though he failed to obtain any informed consent whatsoever from Ms. T for his clandestine activities with the SD5. Ms. Cynthia Stuart exchanged numerous emails with Dr. Todd Kettner and also arranged for a conference call between Dr. Todd Kettner and the School District No. 5 Southeast Kootenay administrators: Ms. Cynthia Stuart, Director of Human Resources; Mr. William (Bill) Gook, Superintendent; and Mr. Glenn Dobie. Following the conference call, Ms. Cynthia Stuart shared, secretly, with Dr. Todd Kettner so called Mr. Glenn Dobie’s investigation reports (two) of Ms. T.
Once Dr. Todd Kettner completed his report, Ms. T and the Union learned that the SD5 secretly provided Dr. Todd Kettner with at least one of Mr. Glenn Dobie’s Reports dated December 9, 2009. Astonishingly, in response to the Union inquiries, Ms. Cynthia Stuart repeatedly lied to the Union, in writing, and falsely claimed that no such reports existed and did not provide them to the Union nor to Ms. T, while having Mr. Glenn Dobie’s reports in her possession and control and distributing them to others, in particular to Dr. Todd Kettner.
When Ms. T arrived to Dr. Todd Kettner’s offices in June 2010, she had no idea about Dr. Todd Kettner’s clandestine activities with the School District No. 5 Southeast Kootaney’s administrators, no idea that Ms. Cynthia Stuart sent Dr. Kettner Mr. Glenn Dobie’s “non-existing” investigation reports, and no idea what was in Mr. Glenn Dobie’s “non-existing” investigation report.
Dr. Todd Kettner’s Administration of the PAI to Ms. T and Dr. Kettner’s Opinion/Conclusion About Ms. T
Dr. Todd Kettner sat Ms. T in front of a computer and asked her to complete a computerized version of the PAI while he went to do something else. Dr. Kettner later printed a computerized report titled “Personality Assessment Inventory: Clinical Interpretive Report” by “Leslie C. Morey, PhD and PAR Staff” (2000); plagiarized a few lines from nearly four pages long interpretive text in the PAI computerized report, and concluded, that the “interpretation of the PAI clinical scales was not appropriate.” The excerpt below shows, in its entirety, Dr. Kettner’s description of the PAI assessment in his June 14, 2010 Report, with the bold text showing verbatim plagiarism and italicized text showing word substitutions and paraphrasing of the content lifted, without acknowledgment, directly from the computerized report.
Questionnaire Results
The Personality Assessment Inventory is a 344-item self-report measure of personality and psychological functioning that has been normed on a population of over 2,000 individuals in clinical and non-clinical settings across North America. Validity indicators of the PAI suggest that Ms. T tended to portray herself in a consistently favourable light and is likely to be unaware of or admit to common shortcomings that most individuals will readily acknowledge. She may thus be unaware of, deny, or repress unfavorable negative consequences of her behavior or the effect that her actions may be having on others. Given this response pattern, which seems to me to be somewhat unconscious lack of insight into her difficulties, further interpretation of the PAI clinical scales was not appropriate.
Dr. Todd Kettner, June 14, 2010 Report
Dr. Todd Kettner appears to have looked at the validity indicators (ICN, INF, NIM, & PIM) and concluded that (a) Ms. T was portraying herself “in a consistently favourable light”, has “common shortcomings” of which she is “likely to be unaware”, “may” “be unaware”, “deny”, or “repress” “unfavorable negative consequences of her behavior” on others. and that (b) her clinical profile was invalid and not to be interpreted.
What did the PAI Interpretive Report say about Ms. T’s “clinical scales”? Dr. Todd Kettner did not mention it in his report, did not plagiarize it, but the PAI Interpretive Report said that Ms. T’s clinical profile was entirely normal.
The PAI clinical profile reveals no elevations that should be considered to indicate presence of clinical psychopathology…
The PAI clinical profile is entirely within normal limits. There are no indications of significant psychopathology in the areas that are tapped by the individual clinical scales…
The PAI Interpretive Report (Morey, 2007, p. 7), generated by Dr. Todd Kettner
Why would Dr. Todd Kettner suppress this most critical result from the PAI assessment? Did Dr. Kettner have an agenda? Was he trying to arrive to the conclusions the SD5 wanted him to arrive to?
Fatal Flaws In Dr. Todd Kettner’s Work
Dr. Todd Kettner did not disclose that he compared Ms. T to 20 years obsolete norms from a foreign country
Dr. Todd Kettner described the PAI as an instrument “normed on a population of over 2,000 individuals in clinical and non-clinical settings across North America.”
In the context of Ms. T’s assessment, Dr. Todd Kettner’s description is at minimum misleading if not outright false. First, as the computerized report generated by Dr. Kettner himself plainly shows, Dr. Kettner used “a census matched standardization sample of 1,000 [not 2,000] normal adults” to calculate Ms. T’s scores. Second, as the PAI Manual (Morey, 2007) shows and as Dr. Kettner must have known (if he was competent and read the PAI manual), the “normative group was a U.S. [not Canadian] census-matched community sample of 1,000 adults…” (p. 25) recruited from only 12 out of 50 US states (p. 79). In other words, Dr. Kettner used the US norms from selected US states, and not Canadian norms to form his opinions about Ms. T’s personality. Third, Dr. Kettner failed to mention that the US norms were established in 1990 or earlier and were at least 20 years outdated and obsolete by the time Dr. Kettner used these US outdated norms to assess Ms. T and to calculate her PAI scores (more precisely, it was a computer rather than Dr. Kettner who assessed Ms. T and calculated her PAI scores). Note that there have never been Canadian norms published for the PAI and that some Canadian clinical psychologists use the US outdated norms as if those norms were applicable to Canadians even today (see Uttl, Sikma, & Tat, 2025).
Dr. Todd Kettner was either unaware that the norms ought to be both current and based on a representative population he intends to use the PAI with (Canadian population), or he intentionally withheld this critically relevant information from readers of his report to cover up his incompetence. College of Psychologists of British Columbia Code of Conduct (2009) clearly informed Dr. Kettner that he ought not to use obsolete tests and tests that are “not applicable to the current purpose.”
11.21 Obsolete/outdated results/tests
College of Psychologists of British Columbia Code of Conduct (2009)
A registrant must not base his or her assessment or intervention decisions or recommendations on
(a) data or test results that are outdated for the current purpose, or
(b) tests and measures that are obsolete and not applicable to the current purpose.
Dr. Todd Kettner also appears unaware of his professional and ethical obligations to clearly state the limitations of his approach/his activities. The key limitation of Dr. Kettner’s approach was that Dr. Kettner had no scientific evidence and no scientific data to inform him how Canadians such as Ms. T and other teachers employed by the SD5 would score on the PAI in 2010 (rather than in 1990) while under threat of loosing her career.
11.11 Reporting limitations in validity or accuracy
College of Psychologists of British Columbia Code of Conduct (2009)
A registrant must
(a) indicate any significant reservations he or she has about the accuracy or the validity of the assessment, or limitations of his or her interpretations in any assessment report, and
(b) include in his or her report of the results of a formal assessment procedure for which norms are available, any limitations of the assessment norms for the individual assessed and any relevant reservations or qualifications which affect the validity, reliability, or other interpretation of results
As the result, Dr. Kettner’s conclusions were no more valid than conclusions one may obtain from a friendly neighborhood tarot card reader or by shaking a Magic 8 Ball.
Dr. Todd Kettner plagiarized “his opinion” from the computerized report
Dr. Todd Kettner apparently had no idea how to interpret the PAI results and so he instead liberally plagiarized most of “his” professional opinions from the PAI computerized report. Obviously, the PAI computerized report does not have a PhD, is not a registered psychologist in British Columbia, was not an expert, had no awareness of Ms. T’s circumstances and the assessment situation, and, is not qualified to give psychological opinions in the province of British Columbia or elsewhere. The software apparently did not even know that Ms. T was a Canadian rather than US woman because “Morey and the PAR staff” did not code it it in.
Moreover, the reliability and validity of the PAI computerized reports has never been established nor transparently and publicly verified for Canadians nor for US population. The PAI Clinical Interpretive Report has also not been peer-reviewed – its magic is hidden in a secret software code that has never been publicly disclosed nor peer-reviewed. Thus, the PAI computerized reports, like computerized reports for other psychological tests, are “black magic.” No one knows how the software generating the reports arrive from the PAI data to the interpretive verbiage, and no one has ever published any study showing that the interpretive verbiage is rationally connected to the PAI scores.
Dr. Kettner is apparently oblivious to his professional and ethical obligations to form his professional opinions himself and plagiarized much of his opinion from the computerized report instead. Alternatively, Dr. Kettner is aware of his professional obligations but choose to ignore them and engage in his copy paste/re-arrange/substitute words plagiarism knowing it was wrong and unprofessional conduct.
11.19 Reliance on computer reports
College of Psychologists of British Columbia Code of Conduct (2009)
A registrant must never substitute computer generated assessment reports or statements for his or her own professional opinion, assessment or report.
11.20 Acknowledgment of sources
A registrant who uses computer-generated interpretive statements in preparing psychological evaluations must
(a) acknowledge the sources of such statements in a written citation that is formally included in the client report, and
(b) formally quote, using an appropriate format, any material taken verbatim from computer-generated interpretations.
In any case, Dr. Todd Kettner is not only self-admitted plagiarist, peddling the PAI Interpretive Report’s opinions as his own, but he is also either unable or unwilling to follow clear practice standards of his profession.
Dr. Todd Kettner failed to consider unreliability of the PAI scores
Scores one may obtain on any psychological test, including the PAI, are imprecise, that is, they are influenced and include error. How large that error tends to be can be determined, for example, by giving the same test to the same group of individuals and calculating the correlations among the two sets of scores. This is called a test-retest reliability. Technically, the reliability, like any other correlation, can range from -1 to +1 with -1 indicating that examinees responded exactly opposite ways on the two administrations, 0 indicating nor relationship between the two administrations’ scores, and 1 indicating a perfect relationship between the two administrations’ scores. In high stakes assessments, a reliability ought to be very high, over .90 or over .95, to avoid basing life changing decisions about examinees on random error (see Uttl, Sikma, & Tat, 2025).
In turn, a reliability of scores determines so called “standard error of measurement” and 95% confidence interval, the interval calculated around an observed scores that tells us we can be 95% confident that the true score lies somewhere in that 95% confidence interval. The PAI Manual (Morey, 2007) states:
The standard error of measurement, expressed in points on the T-score scale, represent the standard deviation of the hypothesized error term as a contribution to observed PAI T-scores. Thus, one can be 95% certain that a participant’s true score on a PAI scale falls within 1.96 standard errors of measurement of his or her observed score…
Morey (2007), The PAI Manual, p. 135 (see also Uttl, Sikma, & Tat, 2025)
Reliabilities of the PAI scores are generally insufficient for the PAI scores to be used in high stakes decisions about individuals (they range from .29 to .94 with only a few exceeding .90 – see Table 8.7 in the PAI manual or Uttl, Sikma, & Tat, 2025). As a result, the standard errors of measurement are quite large, and corresponding 95% confidence intervals are very wide.
Dr. Todd Kettner has neither considered nor mentioned the PAI scores reliability, standard errors of measurements, and 95% Confidence Intervals. If he did, Dr. Kettner would have to arrive to the only possible conclusions: there was nothing wrong with Ms. T as her scores were no different from the scores of the US 1990 normative samples.
The figure below shows the 22 PAI scales, reliabilities, SEms, Ms. T’s scores, 95% Confidence Intervals for Ms. T’s scores, 95% CI span/imprecision, and whether or not each Ms. T’s score was different from the middle 68% of the US 1990 normative sample.
| PAI Scale | rxx | SEm | Ms. T’s score | 95% CI high | 95%CI low | 95% CI Span | Different from the middle 68% |
| ICN | 0.29 | 8.43 | 49 | 65.5 | 32.5 | 33.0 | No |
| INF | 0.43 | 7.55 | 51 | 65.8 | 36.2 | 29.6 | No |
| NIM | 0.71 | 5.39 | 47 | 57.6 | 36.4 | 21.1 | No |
| PIM | 0.81 | 4.36 | 57 | 65.5 | 48.5 | 17.1 | No |
| SOM | 0.86 | 3.74 | 57 | 64.3 | 49.7 | 14.7 | No |
| ANX | 0.88 | 3.46 | 44 | 50.8 | 37.2 | 13.6 | No |
| ARD | 0.85 | 3.87 | 49 | 56.6 | 41.4 | 15.2 | No |
| DEP | 0.91 | 3.00 | 58 | 63.9 | 52.1 | 11.8 | No |
| MAN | 0.85 | 3.87 | 59 | 66.6 | 51.4 | 15.2 | No |
| PAR | 0.88 | 3.46 | 52 | 58.8 | 45.2 | 13.6 | No |
| SCZ | 0.87 | 3.61 | 47 | 54.1 | 39.9 | 14.1 | No |
| BOR | 0.9 | 3.16 | 49 | 55.2 | 42.8 | 12.4 | No |
| ANT | 0.9 | 3.16 | 53 | 59.2 | 46.8 | 12.4 | No |
| ALC | 0.94 | 2.45 | 43 | 47.8 | 38.2 | 9.6 | No |
| DRG | 0.88 | 3.46 | 44 | 50.8 | 37.2 | 13.6 | No |
| AGG | 0.85 | 3.87 | 41 | 48.6 | 33.4 | 15.2 | No |
| SUI | 0.71 | 5.39 | 47 | 57.6 | 36.4 | 21.1 | No |
| STR | 0.88 | 3.46 | 57 | 63.8 | 50.2 | 13.6 | No |
| NON | 0.81 | 4.36 | 42 | 50.5 | 33.5 | 17.1 | No |
| RXR | 0.83 | 4.12 | 53 | 61.1 | 44.9 | 16.2 | No |
| DOM | 0.77 | 4.80 | 61 | 70.4 | 51.6 | 18.8 | No |
| WRM | 0.74 | 5.10 | 70 | 80.0 | 60.0 | 20.0 | No |
When considering the imprecision of the PAI scores, it is obvious that there was nothing wrong with Ms. T and that Dr. Todd Kettner’s disparaging comments about Ms. T, the comments Dr. Todd Kettner plagiarized from the PAI Interpretive Report were nothing but a big pile of nonsense.
Dr. Todd Kettner failed to understand what the PIM (Positive Impression Management) scale actually measures
Dr. Todd Kettner only mentioned “Validity indicators of the PAI” in his one paragraph about Ms. T’s PAI “Questionnaire Results.” The validity indicators are the ICN (Inconsistency), INF (Infrequency), NIM (Negative Impression Management) and PIM (Positive Impression Management) scales. Although Dr. Kettner did not mention it in his June 14, 2010 Report, Dr. Kettner generated the PAI Interpretive Report, plagiarized from it (see above), and hand-circled the PIM score in the profiled printed on the page 2 of the report, and hand-wrote the following next to: “on the defensive b/c of situation.” Ergo, at the time, Dr. Kettner came to conclusion that Ms. T’s PIM score of 57T (57 on T-scale with the mean of 50 and standard deviation of 10) occurred, in part, because Ms. T was “on the defensive b/c of situation.”
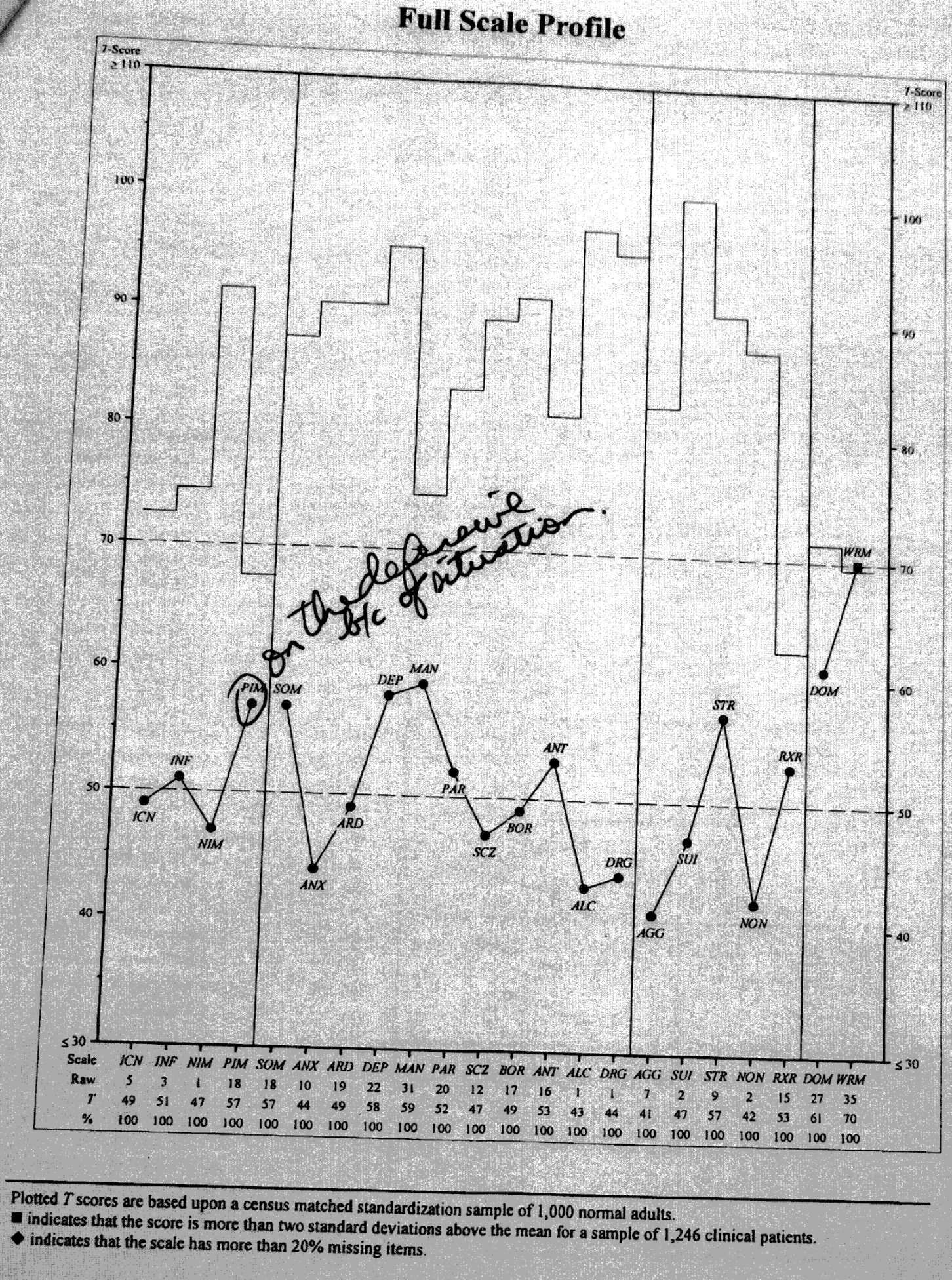
The image above is a copy of the PAI Interpretive Report (Morey, 2000), page 2, showing Ms. T’s Full Scale Profile, with Dr. Kettner’s circle around PIM and his “on the defensive b/c of situation.” As detailed above, this profile, including the PIM, is non-remarkable, that is, perfectly normal when precision of these observed scores is considered (which Dr. Kettner failed to do).
However, let’s focus on the PIM and what it measures.
First, the PIM is unreliable. The 95% Confidence Interval around 57T PIM ranges from 48.5 to 65.5, meaning Dr. Kettner ought to have known that Ms. T’s PIM of 57T was no different from the average of the US 1990 normative sample (i.e., 50T). Hence, Dr. Kettner had no basis for his disparaging comments about Ms. T’s awareness, shortcomings, defensiveness, etc. that he plagiarized from the PAI Interpretive Report.
Second, if Dr. Todd Kettner read the PAI Manual, Dr. Kettner would have learned that the PIM actually does not measure only the positive impression management but that it also measures perfectly truthful and accurate responding.
The PAI Manual states (Morey, 2007):
… There are a number of reasons why people completing a self-report instrument might not report negative characteristics. One possibility is that the respondent indeed does not have negative characteristics [the instrument asked about], or at least has fewer than most individuals. A second possibility is that they are not telling the truth—that they are trying to deceive… A third possibility is that they are simply not aware of certain faults that they may have… It is these later two characteristics that PIM was designed to measure.
Morey (2007, p. 30), PAI Professional Manual 2nd Edition
Since the PAI PIM measures both honest/truthful responding — for respondents who do “not have negative characteristics, or at least has[ve] fewer than most individuals” — and positive impression management (what some psychologists call “faking good”), the PIM is (a) mis-named and (b) invalid measure of any particular construct including the positive impression management. An interested reader can examine Uttl, SIkma, and Tat (2025) for more comprehensive discussion of the PAI, including the PAI PIM scale. With respect to the PAI PIM (Positive Impression Management) scale, we concluded the following:
If the index identifies honest examinees as “faking good”, the index is wrong, inappropriate, and its use in any high or even low stakes assessments is unconscionable and unethical. Labelling an examinee as dishonest, as “faking good”, is a severely defamatory accusation. No psychologist should ever make a claim that the examinee is dishonest when the psychologist has no idea what caused the particular score, has no idea about the errors of measurement, and has no idea how to interpret psychological scores. The severity of this relevant non-disclosure by psychologists is further compounded by the fact that a reader of a psychological report who is not a psychologist and not an expert (a) has no indication that they were misled, and (b) has no way to access the test manual to find out that they were misled about the PIM since only qualified psychologists can access the PAI manual but the public can not.
Uttl, Sikma, & Tat (2025)
The PAI’s PIM is not only unreliable and invalid measure of anything, the PIM 57T cutoff (2/3 standard deviation above the mean of the US 1990 normative sample) recommended by Morey (2007) and blindly used by Dr. Kettner, but also misclassifies a large percentage of normal examinees (normative sample) as “faking good” or engaging in “positive impression management.” Morey (2007) was fully aware of this issue and explains:
It should be recognized that the tendency for favorable self-presentation appears to be fairly common in the normal population. Typically, most cutoff scores on indexes of social desirability that were derived from clinical studies will identify 30% to 40% of the general population as “faking good.” Such results underscore the difficulty of distinguishing defensive responding from normality with respect to clinical instruments…
Morey (2007, p. 30), PAI Professional Manual 2nd Edition
Unfortunately, Morey’s (2007) admissions are nowhere to be found in the PAI Interpretive Report. Ms. T’s PAI Interpretive Report made no mention that (a) the PIM 57T may be because Ms. T “does not have negative characteristics [the instrument asked about], or at least has fewer than most individuals” and/or that (b) the PIM mis-classifies large percentage of normal, non-faking people as “faking good”, “dishonest” or “defensive.”
In any case, as detailed above, Dr. Todd Kettner had no scientific reason to believe that Ms. T was “faking good”, had “shortcomings” and was unaware of them, was “defensive”, etc..
Dr. Todd Kettner ignored base rates of “abnormal” scores
It is a well known, elementary fact in statistics and in psychological testing literature that more opportunities there are for an “abnormal” scores to appear, more abnormal scores will be observed. Take an ordinary six faced die and consider what is a likelihood of obtaining “elevated” or “high” score of 6. If you roll a die once, you will observe the high score of 6 with the probability 1/6 or .17, approximately. If you roll a die 22 times, you will observe at least one high scores of 6 in 22 rolls with the probability near 1.0. The same is true for psychological test scores. For tests such as the PAI, a chance that one will observe at least 1 abnormal/elevated/high score due to chance across the 22 scales is close to 1.0. Multivariate base rates of high or abnormal scores tell a psychologists how many high or abnormal scores the psychologist can expect by chance alone among a specific number of test scores.
The PAI Interpretive Report (Morey, 2000) gives an ignorant or unscrupulous psychologists over 100 scores to sift through for “abnormal” scores, most of them with no evidence of their reliability or validity. The available scores are: 22 PAI Scale Scores (rxx range = .29 to .94), 31 PAI Subscale Scores (rxx range = .67 to . .86), 10 Supplemental PAI Indexes (no reliabilities reported), and 43 Coefficients of Fit (correlations with samples of various groups). Accordingly, a psychologist has at least 106 scores to sift through and examine for “abnormal” scores, and, statistically, it is nearly certain that there will be at least 1 abnormal scores (and likely many more) present due to chance alone.
Dr. Todd Kettner did not mention multivariate base rates of abnormal scores, and apparently, was oblivious to what multivariate base rates are. Similarly, the PAI Interpretive Report (Morey, 2000) is also silent about multivariate base rates. Perhaps not surprisingly, the PAI Professional Manual 2nd Edition (Morey, 2007) is also silent and does not mention multivariate base rates.
Dr. Todd Kettner withheld information undermining his opinions and conclusions about Ms. T
Dr. Todd Kettner kept his opinion that Ms. T’s PIM 57T scores indicated Ms. T was “on defensive b/c of the situation” to himself and chose not to disclose it in his June 14, 2010 Report. On a witness stand and under oath, more than a decade later, Dr. Todd Kettner admitted that he himself made that handwritten note that he did not mention in his report.
Why is this important?
It is well known in psychological testing literature that when a psychologist compares an examinee to some normative data, the normative data ought to be based on performance of examinees in the same situation and drawn from the same population. Accordingly, the norms differ among countries (e.g, US vs. Canada but they also differ among, for example, between situations. Specifically, examinees who are asked to take the PAI while applying for jobs will naturally not be disclosing their minor shortcomings or negative characteristics even if they have them. Weiss (2010) explained this succinctly and noted that “the evaluating psychologist should not label a profile as extremely defensive or deceptive unless the PIM score is extraordinarily elevated.”
An important issue in interpreting PIM with job applicants is that the job applicant scenario appears to “pull” for elevated scores on validity scales related to positive self-presentation (Roberts et al., 2004; Weiss, Weiss, Cain, & Manley, in press). Such applicants will tend to obtain higher scores on measures of defensiveness and positive impression management, such as the PAI PIM scale, and the L and K scales on the MMPI-2, than will individuals given the test for other purposes. This is because the pre-employment situation encourages applicants to present themselves in a positive light to a much greater degree than they would normally. Therefore, higher cutoff scores should be used to determine levels of defensiveness (see for example Weiss et al., in press). Roberts et al. (2004) make the point that elevated scores on PIM (T = 70 in one of the sample cases presented) are within the normal range for law enforcement and public safety applicants. Therefore, the evaluating psychologist should not label a profile as extremely defensive or deceptive unless the PIM score is extraordinarily elevated.
Weiss, P. (2010), “Using of the PAI in Personnel Selection”, in Blais, M.A., Baity, M.R., & Hopwood, C.J. (2010). Clinical Applications of the Personality Assessment Inventory, Routledge.
Ms. T’s PIM of 57T (a) was not elevated relative to the US 1990 norms, (b) was most certainly not elevated relative to samples of job applicants, and (c) was most certainly not elevated relative to samples of examinees whose are sent for testing because their employers wants to fire them.
Was Dr. Todd Kettner so incompetent that he failed to realized the significance of his insight that the PIM 57T could be due to “situation”? Or did he realize the significance and chose to keep it secret — to suppress it and, to use his term, to repress it — to make the School District No. 5 happy and to make Ms. T appear “unaware” of her “shortcomings” etc..?
Conclusions
Dr. Todd Kettner’s assessment of Ms. T was fatally compromised at every stage and cannot be considered legitimate in any professional or scientific sense. Before Ms. T ever met him, School District No. 5 Southeast Kootenay initiated secret, ex-parte communications with Dr. Kettner, supplied him with internal investigation reports they falsely claimed did not exist, and discussed Ms. T behind her back and without her consent with Dr. Kettner. These clandestine exchanges destroyed any possibility of neutrality or independence. By participating in these undisclosed communications, Dr. Kettner abandoned his ethical obligations, disregarded Ms. T’s right to informed consent, and aligned himself with the agenda of her employer, School District No. 5 Southeast Kootenay, rather than the standards of his profession.
Methodologically, Dr. Todd Kettner’s conduct represents a profound breakdown of professional competence. Instead of performing a genuine psychological assessment, Dr. Todd Kettner relied on a computer-generated PAI Interpretive Report, copied substantial portions of it without attribution, and substituted algorithmic, computer generated text for his own professional judgment. Dr. Todd Kettner suppressed the most important clinical finding—that Ms. T’s PAI profile was entirely normal—and instead advanced an unfounded claim of “positive impression management.” Dr. Kettner’s interpretation ignored basic psychometric principles, including measurement error, reliability, situational context, multivariate base rates, and the inevitability of chance elevations. Compounding these failures, Dr. Kettner used decades-old U.S. norms, misrepresented them as “North American,” and withheld their limitations from the reader.
The result is clear: Dr. Todd Kettner’s assessment was neither objective, nor ethical, nor scientifically defensible. Dr. Kettner’s conclusions are unsupported by the data, distorted by undisclosed conflicts, and rendered meaningless by profound methodological errors. No responsible decision-maker should have relied on this assessment for any purpose, let alone high-stakes decisions affecting Ms. T’s career and reputation.
Was Dr. Todd Kettner incompetent, was he malicious/did he intent to harm Ms. T, or did he take on a role of the School District No. 5’s hired gun, hired assassin?
The first explanation, Dr. Todd Kettner‘s incompetence, is consistent with the fact but does not explain Dr. Kettner’s secret, repeated ex-parte communications with the SD5, omission of the most critical finding (normal clinical profile), suppression of his own view evidenced by his handwritten note about situational defensiveness, and Dr. Kettner’s consistent one-sided interpretation favouring the SD5 position and harming Ms. T. Notably, these are not mere technical or procedural errors as they involve intentional, selective behavior.
The second explanation, Dr. Todd Kettner‘s malice/intent to harm Ms. T, is also consistent with the facts and supported by Dr. Kettner withholding findings favourable to Ms. T, framing normal results as pathological, and secretly accepting the SD5 information about Ms. T without her knowledge and consent. Thus, malice explanation for Dr. Kettner’s conduct is definitely possible but there appears to be no personal, ideological, or emotional motive for Dr. Kettner to seek harm to Ms. T.
The third explanation, Dr. Todd Kettner accepting the role of the SD5’s hired gun or hired assassin appears to be the most likely. A “hired gun” psychologist (a) aligns their conclusion with the interests of the party seeking the assessment, (b) accepts or solicits ex-parte information, (c) downplays or ignores evidence that contradicts the desired narrative, (d) frames ambiguous or normal results as abnormal or pathological, and (e) provides reports that serve administrative or legal objectives of the hiring party. This matches Dr. Kettner’s behavior:
- The SD5/employer initiated secret contact with Dr. Kettner
- Dr. Kettner participated without Ms. T’s informed consent
- Dr. Kettner received secret documents from the SD5
- Dr. Kettner’s conclusion aligned with the SD5 interests
- Dr. Kettner omitted and supresed findings favourable to Ms. T
- Dr. Kettner’s methodological choices consistently skewed the results against Ms. T
Thus, the most plausible explanation, given Dr. Kettner’s pattern of conduct, is that Dr. Todd Kettner took on a role of a hired-gun/hired assassin, whether consciously or unconsciously, rather than acting independently as a neutral and ethical assessor.